




Clinical record
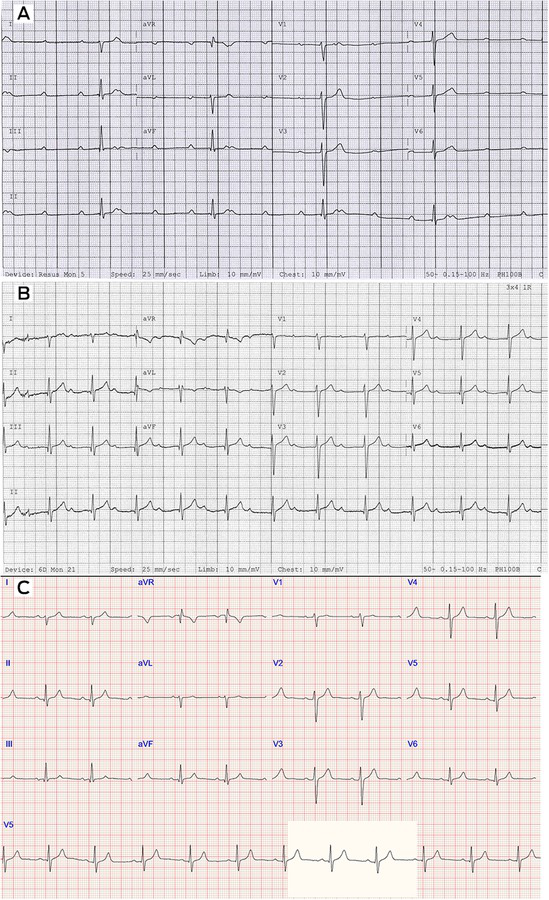
A well 37‐year‐old male patient presented to a tertiary hospital in New South Wales in July 2024 with presyncope and his smart watch alerts indicating resting bradycardia at 40 beats per minute (bpm). He reported one week of upper respiratory tract infection symptoms before presentation. Ambulance electrocardiogram (ECG) showed complete heart block (CHB). Despite escalating isoprenaline infusion (50 μg/hr to 140 μg/hr), he remained intermittently in CHB and high grade atrioventricular (AV) block with persistent presyncope (Box 1, A).
His medical history included seronegative, inflammatory arthritis that was localised to his hands and well controlled on long term methotrexate. There was no family history of sudden cardiac death. Several family members had previously undergone pacemaker implantation between the ages of 50 and 70 years. He was a non‐smoker and consumed occasional alcohol socially.
On presentation, he was afebrile and hemodynamically stable on isoprenaline infusion. There were no rashes noted. Cardiovascular, respiratory, gastrointestinal and rheumatological examinations were within normal limits. Initial blood tests were within normal reference ranges.
His transthoracic echocardiogram showed normal biventricular function and no significant valvular abnormalities. Cardiac magnetic resonance imaging found normal biventricular size and systolic function, with no late gadolinium enhancement, scarring or evidence of myocardial infiltrative disorders. Positron emission tomography/computed tomography found no significant fluorodeoxyglucose uptake in the ventricular myocardium to suggest cardiac sarcoidosis, although mild uptake at the mitral annulus was noted (unclear significance) and fluorodeoxyglucose‐avid nodes in the bilateral axillae were likely indicative of an inflammatory response to a recent respiratory illness.
The patient remained in CHB with an isoprenaline infusion requirement to maintain a stable junctional escape rhythm.
The patient was consulted by a cardiac electrophysiologist. On taking a travel history, it came to light that the patient had recently hiked in the northeastern United States during a work trip two months before presentation, during which he experienced tick bites. He subsequently developed a large rash on his trunk that resolved without treatment. During his subsequent travels, he also hiked in other countries including Spain, Canada and Vanuatu. Considering this history, Lyme disease serology was tested, and the decision for pacemaker insertion was deferred until this diagnosis was excluded.
Serology confirmed Borrelia burgdorferi lgG and lgM positivity. Intravenous ceftriaxone was initiated, leading to progressive improvement in conduction with an ECG after one dose demonstrating AV Wenckebach. Isoprenaline was weaned over two days, and the ECG showed sinus rhythm with 1:1 conduction, albeit with a left posterior fascicular block and first degree heart block (PR interval 310 ms) (Box 1, B).
While polymerase chain reaction testing for Lyme Borrelia DNA was not detected, the clinical presentation of reversible CHB and positive serology is consistent with Lyme carditis.
Before discharge, a stress echocardiogram reassuringly demonstrated 1:1 atrioventricular conduction throughout, up to a peak heart rate of 180 bpm. The patient was discharged under hospital‐in‐the‐home service to complete a four‐week course of intravenous ceftriaxone as advised by the infectious disease team. Weekly follow‐ups with ECGs confirmed that he remained in sinus rhythm with a normalised PR interval (Box 1, C).
Discussion
Lyme carditis, first described in 1980, is an early systemic manifestation of Lyme borreliosis caused by Borrelia burgdorferi sensu lato spirochetes.1,2 It typically occurs within one to two months of infection.2,3 Endemic in temperate regions of the northern hemisphere, Lyme carditis frequently presents with fluctuating AV block, although less commonly as myocarditis, pericarditis, valve disease, or tachyarrhythmias.3 Up to 90% of patients with Lyme carditis develop a degree of heart block, and around two‐thirds of these heart block cases present with high degree AV block including Mobitz type II and third degree block.4 About 40% of cases have the distinctive erythema migrans rash.5
Diagnosis can be challenging due to the variable presentation of Lyme carditis, and tools, such as the Suspicious Index in Lyme Carditis (SILC) risk score6, aid in risk stratification for undifferentiated patients with heart block6 (Box 2). Early treatment and prompt initiation of empiric antibiotics (oral doxycycline for mild cases and intravenous ceftriaxone for severe cases) are critical in confirmed or suspected cases to reduce morbidity.3,5 In rare instances, patients with persisting symptomatic high degree AV block have been managed with a temporary–permanent pacemaker to support recovery and facilitate earlier discharge from hospital.7,8
This case is particularly notable as Lyme carditis is rarely diagnosed in Australia. To our knowledge, there have been no locally acquired Borrelia burgdorferi cases in Australia, and absence of its tick vectors suggests that Lyme disease is not endemic in Australia.9 This highlights the importance of considering Lyme carditis as a differential diagnosis for unexplained heart block, especially in young patients and returning travellers, given its reversibility and good prognosis with early initiation of antibiotics.
Lessons from practice
- Lyme disease is the most common tickborne illness in North America and although not endemic in Australia, should be considered in all returning travellers from endemic regions.
- Lyme carditis is frequently associated with high degree AV conduction abnormalities, and carries a favourable prognosis with prompt initiation of antibiotic therapy.
- Early consideration and recognition of Lyme carditis is crucial because it is a highly reversible condition, potentially averting the need for permanent pacemaker insertion if treated promptly.
Box 1 – (A) Admission electrocardiogram (ECG) showing complete heart block, junctional escape approximately 30 beats per minute. (B) Day 7 of admission: few hours after first dose of ceftriaxone. ECG showing sinus rhythm with first degree heart block (PR interval 310 ms) and right axis deviation. (C) Two weeks after ceftriaxone: right axis deviation persists, sinus rhythm with normalised PR interval (160 ms) at hospital‐in‐the‐home clinic review
Box 2 – Suspicious Index in Lyme Carditis (SILC) score and COSTAR mnemonic6: a total score of 0–2 indicates low risk, 3–6 indicates intermediate risk and 7–12 indicates high suspicion of Lyme carditis
|
Variable |
Value |
||||||||||||||
|
|
|||||||||||||||
|
Constitutional symptoms* |
2 |
||||||||||||||
|
Outdoor activity/endemic area |
1 |
||||||||||||||
|
Sex = male |
1 |
||||||||||||||
|
Tick bite |
3 |
||||||||||||||
|
Age < 50 years |
1 |
||||||||||||||
|
Rash = erythema migrans |
4 |
||||||||||||||
|
|
|||||||||||||||
|
* Fever, malaise, arthralgia and dyspnoea. |
|||||||||||||||
Provenance: Not commissioned; externally peer reviewed.
- 1. Steere AC, Batsford WP, Weinberg M, et al. Lyme carditis: cardiac abnormalities of Lyme disease. Ann Intern Med 1980; 93: 8‐16.
- 2. Shah R, Kanzaria M. A case series of Lyme carditis with complete heart block. The Medicine Forum 2012; 13: Article 4. Thomas Jefferson University.
- 3. Yeung C, Baranchuk A. Diagnosis and treatment of Lyme carditis: JACC Review Topic of the Week. J Am Coll Cardiol 2019; 73: 717‐726.
- 4. Wan D, Blakely C, Branscombe P, et al. Lyme carditis and high‐degree atrioventricular block. Am J Cardiol 2018; 121: 1102‐1104.
- 5. Centers for Disease Control and Prevention. Lyme disease. United States Government, CDC, 2022. https://www.cdc.gov/lyme/index.html (viewed Feb 2025).
- 6. Besant G, Wan D, Yeung C, et al. Suspicious index in Lyme carditis: systematic review and proposed new risk score. Clin Cardiol 2018; 41: 1611‐1616.
- 7. González MD, Bianco M, Patel M. Treating Lyme carditis high‐degree AV block using a temporary–permanent pacemaker. Ann Noninvasive Electrocardiol 2017; 22: e12599.
- 8. Aromin C, Chanda A, Kumar S, Thomas GR. A practical ambulatory approach to atrioventricular block secondary to Lyme carditis. J Innov Card Rhythm Manag 2023; 14: 5365‐5368.
- 9. Russell RC. Lyme disease in Australia: still to be proven! Emerg Infect Dis 1995; 1: 29‐31.
Patient consent:
The patient provided written consent for publication.
No relevant disclosures.
Author contributions:
Chuah E: Conceptualization, data curation, resources, visualization, writing – original draft, writing – review and editing. Sritharan H: Conceptualization, visualization, writing – review and editing. Seidman Z: Conceptualization, data curation, resources, visualization, writing – review and editing. Ekmejian AA: Conceptualization, supervision, validation, writing – review and editing.Chia K: Conceptualization, supervision, validation, writing – review and editing.