




Why should MJA readers, many of whom are general practitioners, specialists and doctors in training, care about early childhood learning? Because the foundations of lifelong health are laid by school entry, and high quality early childhood education and care (ECEC) is a powerful health intervention.1 High quality ECEC — physically safe, emotionally supportive, intellectually stimulating, predictable and responsive, akin to a nurturing home environment2 — can improve cognitive, emotional, social and behavioural development, reduce long term risks of poor mental health, obesity and chronic disease, and help close equity gaps across the life course.3,4,5,6,7,8,9 Such issues are also high in public consciousness, with recent abuse cases in childcare centres drawing national attention,10 new July 2025 legislation giving the federal government power to suspend or cancel Child Care Subsidy approvals for services failing standards (around 30 currently at risk),11 and a major federal review under way to analyse pricing and delivery models for a universal childcare system.12,13
Health professionals regularly see the effects when children lack optimal early environments at home or in the community, but have few tools to reverse them. For children with chronic illness, missed early learning can deepen lifelong disadvantage.14 As Australia expands its ECEC systems, the health care community has a vital role in understanding, championing and influencing them, guided by high quality causal research on what works, for whom, when and how, while navigating the sector’s diverse governance, workforce pathways and variable quality.
Despite substantial Australian and international work linking ECEC to improved health and developmental outcomes,3,4,5,6,7,8,9 the most effective interventions at population scale remain unclear. This is a fundamental question for a system now receiving multibillion‐dollar investment to increase access, with a current $3.4 billion and suggested additional $1 billion from the Commonwealth government.15 This perspective article is part of the 2025 Future Healthy Countdown 2030 supplement16 and addresses new opportunities to achieve this.
Early brain development underscores what is at stake. It can be likened to the birth of a star — an extraordinary, brief and critical phase that, largely hidden from view, sets the scene for all that follows. In the first 1000 days, over one million new neural connections form each second, building the brain’s foundational architecture. In the next 1000 days, these networks are sculpted through pruning, shaped by the child’s experiences and environment.17 Like star formation, this developmental process is powerful yet fragile. Once set in motion, it becomes progressively harder to change; for example, the 20% of children with the lowest brain executive functioning by age three years comprise close to 80% of adults needing some form of social or economic assistance.18 This makes early childhood not just important but the most cost‐effective and impactful period to invest in lifelong health, learning and social outcomes.19
Policy responses
Recognising the importance of the first five years, Australian governments have acted. Since 2008, the federal Universal Access to Early Childhood Education initiative has funded 15 hours of preschool for the year before school.20 The Child Care Subsidy improved affordability, while the 2023 Building Early Education Fund and the Early Childhood Care and Development Policy Partnership targeted infrastructure and equity.21,22,23 Paid parental leave evolved from no national scheme in the early 1990s to 18 weeks for primary carers in 2011, with expansion to 26 weeks by 2026 and including paid partner leave.24 Together, these policies reflect a national commitment to supporting early development through enriched environments and parental engagement.
States are building on this platform in different ways. For example, Victoria has led ambitious reforms, introducing funded Three‐Year‐Old Kindergarten from 2019 and planning a universal 30‐hour Pre‐Prep year by 2036,25 despite workforce and budget constraints. This is complemented by the School Readiness Funding initiative, also introduced in 2019, which provides early childhood centres with between $2000 and $400 000 annually,26 depending on demographic profile, to support educators and families to improve children’s outcomes in communication, wellbeing and inclusion. Western Australia has taken a more targeted approach, aligning with the National Quality Framework and investing in regional and Aboriginal community services.27 These examples reflect a cultural shift: early childhood is increasingly recognised as a shared responsibility across health, education and family systems.
Lessons for ECEC from early school literacy evidence
The journey of literacy teaching offers important lessons. Over the past two decades, international evidence established that systematic phonics instruction (ie, explicit, structured teaching of letter–sound relationships) substantially improves early reading outcomes, especially for disadvantaged children.28,29,30 Australia, however, was slow to adopt this evidence, with whole language and balanced literacy approaches dominating for years despite weaker Grade 3 outcomes. Only recently have most states, prompted by national reviews and international benchmarking declines for Australian children,31 moved toward mandated phonics‐based instruction in the early school years.
This hard‐won, evidence‐driven shift contrasts with early childhood education before school. Here, although ECEC can improve outcomes when of sufficient quality, the evidence base for specific interventions remains weaker and less embedded in policy — what to teach, how to structure environments, how to personalise learning and how implementation of these ingredients can be supported in diverse contexts. Activities such as dialogic reading (ie, shared reading where the adult encourages the child to participate in the storytelling), phonological awareness games, early maths talk, and emotional self‐regulation activities show promise, but causal evidence linking specific preschool practices to later academic and health trajectories is sparse to such an extent that their value can be questioned.32 It would be a major lost opportunity if this lack of specificity as to the “how” and “what” of ECEC diluted the benefits of these major policy investments, rather than being seized as the not‐to‐be‐missed opportunity to build the knowledge base that young children deserve.
Structural challenges to measuring impact
However, such research faces structural challenges. First, research on child development remains siloed. In Australia, biomedical and clinical research is funded by the National Health and Medical Research Council and the Medical Research Future Fund, while the Australian Research Council spans education, social science and economics. New Zealand, the United States, Canada and the United Kingdom have similarly parallel structures. Although each stream has produced important domain‐specific discoveries, they hamper the generation of integrated evidence needed to tackle real‐world early childhood challenges, where health, education and environment converge. This is often reflected in studies not being able to integrate health and non‐health (eg, academic) outcomes, as the funding dictates the type of outcomes that are expected. For instance, the Australian Research Council requires projects to explicitly justify any inclusion of health measures in grant proposals.33 Some countries are taking steps to redress this. In the UK, the Medical Research Council and the Economic and Social Research Council are collaborating on Population Research UK (PRUK) to enhance data interoperability, access and collaboration across disciplines.34 Horizon Europe funds integrated, interdisciplinary research across major societal challenges.35 Australia has yet to take comparable structural action.
Second, the evidence base for preventive care in general lags far behind need due to a paucity of experimental evidence, especially for children.36 Stand‐alone randomised controlled trials, the gold standard for causal inference, are typically slow, costly and difficult to generalise or translate.37 Most occur in clinical samples that are poorly suited for prevention,38 and few achieve the scale (≥ 5000 participants) that would generate precise, policy‐relevant estimates, including for diverse groups and for harms or less common benefits.39 This gap is even starker for children; not only are they under‐represented in trials generally, but very large trials represent just 0.5% of paediatric trials registered internationally. We believe that this gap is ripe to be redressed via today’s early childhood cohorts that are designed both for trials and natural experiments at population scale.40
The opportunity: GenV and ORIGINS case studies
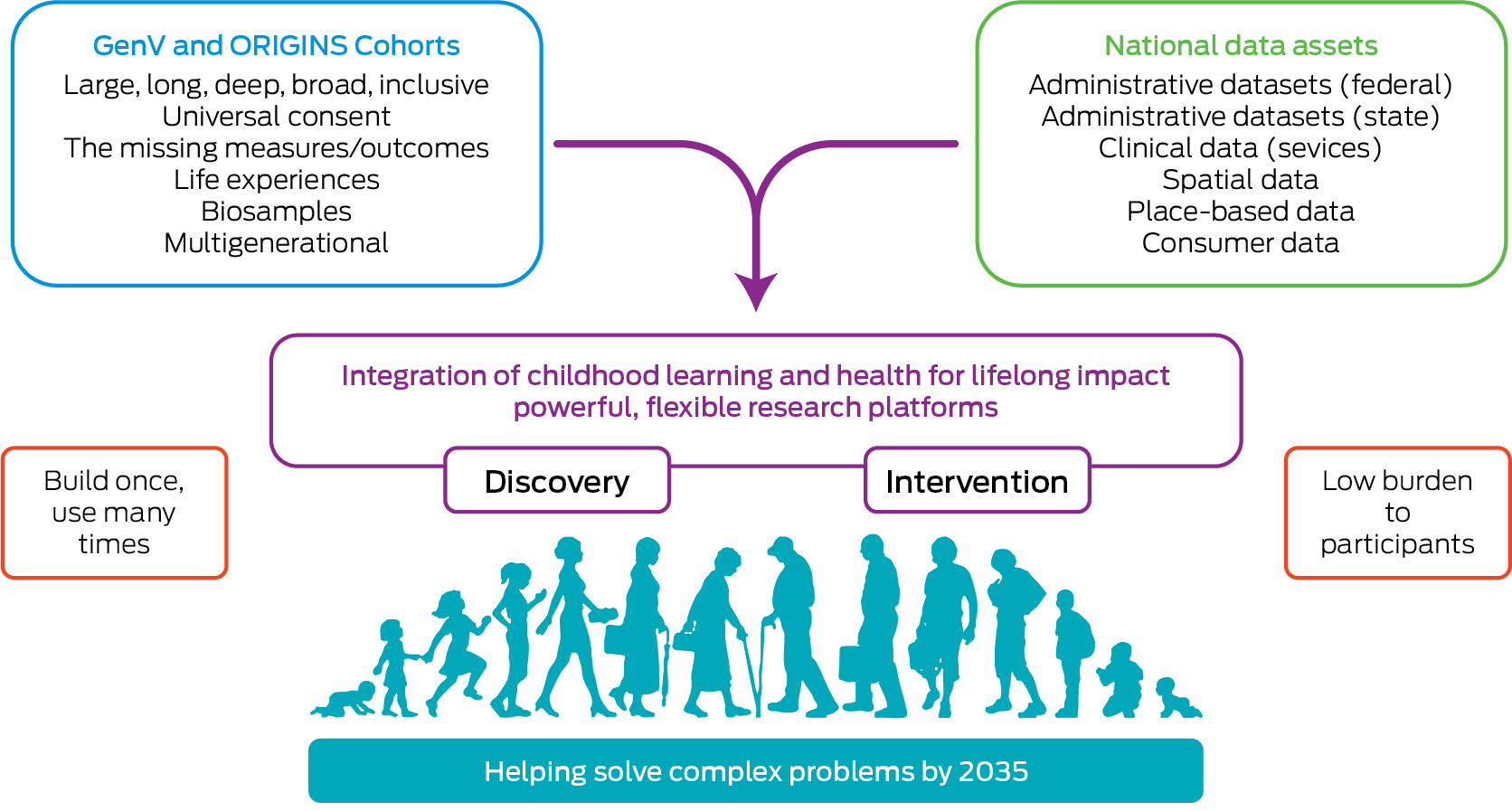
Australia is uniquely well positioned to lead this next generation of research. It has relatively rich observational evidence from the past two decades on ECEC quality and environments (such as the Longitudinal Study of Australian Children,41 E4Kids,42 PLAYCE43) and a body of cluster randomised controlled trials that are strongest in physical activity and self‐regulation (such as AEL,44 PRSIST45) but less informative as to the impacts of policy and changing quality standards. New research designs and intervention‐within‐cohort infrastructures now make it possible to generate robust causal evidence on these issues at population scale, including in early childhood. Two major birth cohorts of the 2020s (ie, Generation Victoria [GenV] and ORIGINS) provide longitudinal, linked and intervention‐ready platforms capable of testing causal pathways, scalable models and multisystem outcomes (Box).
GenV46 is Australia’s largest‐ever birth cohort (≈50 000 children born from October 2021 to October 2023 and ≈75 000 parents), representing all Australian early childhood demographics except remote locations. Its universal data ecosystem is drawing together molecular, subjective experiential and opinion‐based reporting, phenotypic, service, environmental and administrative data (such as the national Personalised Level Integrated Data Asset [PLIDA]) across all 78 local government areas, enabling trials and natural experiments embedded in real‐world early childhood reforms. With 30% of the state’s entire birth cohort participating, GenV is the world’s first true population‐scale, reuse infrastructure designed explicitly for large‐scale interventional preventive research, both universal and targeted.
ORIGINS,47 a single‐community cohort study in Western Australia (≈10 000 children born in 2017–2023 and approximately 12 000 parents), is complementary to GenV: it provides deeper phenotyping, biosamples and engagement to date, enabling over 50 embedded studies (observational and interventional) with a particular focus on mental health, neurodevelopment and place‐based research. Where GenV has breadth, ORIGINS explores more fine‐grained pregnancy and early years data in the city of Joondalup, collecting rich information on social and cognitive development, parenting, kindergarten and school readiness with options for referral to appropriate supports if children are not meeting developmental milestones.
Separately and in collaboration, GenV and ORIGINS are uniquely positioned to evaluate the effects of early learning policies, health interventions and their interactions, capturing the real experiences of today’s young Australian children as they intersect with Australia’s major preschool reforms. For example, the natural variation in Victoria’s phased rollout of the Three‐Year‐Old Kindergarten program and expanded preschool hours offers a rare global opportunity for causal evaluation of ECEC at population scale, especially if GenV can capture not only the relevant whole‐of‐childhood outcomes but the dose and specific components of ECEC delivery across centres. Although GenV does not itself undertake direct observation of ECEC quality, it can link to observational data collected in embedded trials and/or depth cohorts or by services or regulators in routine care, enabling long term outcome evaluations without duplicating assessment. ORIGINS and Edith Cowan University are examining factors that shape school readiness by linking family, medical and developmental data from the first 2000 days with speech and language outcomes at age five years. As these children enter school, both cohorts will similarly be well positioned to assess the impacts of future reforms such as the Australian Government’s 2025–2034 Better and Fairer Schools Agreement,48 which prioritises student wellbeing alongside equity, excellence and workforce development, on connected health, learning and mental health outcomes. As well as these natural experiments, both studies are developing their early life randomised controlled trials capabilities and priorities.49
Conclusion
With lifelong health and opportunity shaped by early‐life experiences and increasingly divergent, the case for bridging the biomedical–social divide has never been stronger. High quality, integrated early life research can move us beyond patchwork knowledge to solutions that reflect the real lives of children and families.
To achieve this, funding bodies must also evolve. Some funding sources, such as UK Research and Innovation (UKRI) and Horizon Europe, are already supporting joint calls and shared infrastructure across disciplines.34,35 If Australia’s funding structures were enabled to support cross‐council collaboration and to reward integrated, preventive longitudinal population infrastructure, we could move from studying disparate pieces to solving a shared puzzle. Greater collaboration, transdisciplinary approaches, integrated service models and medical adoption of child‐centred and trauma‐informed practices from ECEC could strengthen this integration.
The lessons of early literacy reform show that strong evidence, when acted upon, drives better outcomes. By bringing together rapid ECEC reforms with unique, embedded cohorts (GenV and ORIGINS), Australia offers a globally unprecedented opportunity to unite rigorous early education and health research and practice at scale for lasting child wellbeing and population health.
Provenance: Not commissioned; externally peer reviewed.
- 1. Hahn RA, Barnett WS. Early childhood education: health, equity, and economics. Annu Rev Public Health 2023; 44: 75‐92.
- 2. Donoghue EA; Council on Early Childhood. Quality early education and child care from birth to kindergarten. Pediatrics 2017; 140: e20171488.
- 3. Rankin P, Staton S, Jones A, et al. Linking quality and child development in early childhood education and care: technical report. Australian Education Research Organisation, 2024. https://www.edresearch.edu.au/research/technical‐papers/linking‐quality‐and‐child‐development‐early‐childhood‐education‐and‐care (viewed Aug 2025).
- 4. Yoong SL, Lum M, Wolfenden L, et al. Healthy eating interventions delivered in early childhood education and care settings for improving the diet of children aged six months to six years. Cochrane Database Syst Rev 2023; (6): CD013862.
- 5. Grady A, Lorch R, Giles L, et al. The impact of early childhood education and care‐based interventions on child physical activity, anthropometrics, fundamental movement skills, cognitive functioning, and social‐emotional wellbeing: A systematic review and meta‐analysis. Obes Rev 2025; 26: e13852.
- 6. Tonge KL, Mavilidi M, Jones RA. An updated systematic review of correlates of children’s physical activity and sedentary time in early childhood education services. Child Care Health Dev 2024; 50: e13265.
- 7. Blewitt C, Fuller‐Tyszkiewicz M, Nolan A, et al. Social and emotional learning associated with universal curriculum‐based interventions in early childhood education and care centers: a systematic review and meta‐analysis. JAMA Netw Open 2018; 1: e185727.
- 8. Dong X, Burke MD, Ramirez G, et al. A meta‐analysis of social skills interventions for preschoolers with or at risk of early emotional and behavioral problems. Behav Sci (Basel) 2023; 13: 940.
- 9. Morales JS, Alberquilla Del Río E, Valenzuela PL, Martínez‐de‐Quel Ó. Physical activity and cognitive performance in early childhood: a systematic review and meta‐analysis of randomized controlled trials. Sports Med 2024; 54: 1835‐1850.
- 10. Lyons K, Martin S, Belot H. Thousands of reports of abuse have been made in Australian childcare centres. Most alleged perpetrators were allowed to keep working. The Guardian 2025; 28 July. https://www.theguardian.com/australia‐news/2025/jul/28/thousands‐of‐reports‐of‐abuse‐have‐been‐made‐in‐australian‐childcare‐centres‐most‐alleged‐perpetrators‐were‐allowed‐to‐keep‐working (viewed Sept 2025).
- 11. Borys S. Names released of 29 failing childcare centres at risk of losing funding, with more expected to follow. ABC News 2025; 20 Aug. https://www.abc.net.au/news/2025‐08‐20/names‐published‐childcare‐centres‐failing‐standards‐funding/105677954 (viewed Sept 2025).
- 12. Australian Government Department of Education. Notice given to early childhood education and care services not meeting standards [website]. Canberra: Commonwealth of Australia, 2025. https://www.education.gov.au/early‐childhood/announcements/notice‐given‐early‐childhood‐education‐and‐care‐services‐not‐meeting‐standards (viewed Sept 2025).
- 13. Australian Government Department of Education. Early Education Service Delivery Prices project [website]. Canberra: Commonwealth of Australia, 2025. https://www.education.gov.au/early‐childhood/about/strategy‐and‐evaluation/service‐delivery‐price (viewed Sept 2025).
- 14. Peterson JW, Loeb S, Chamberlain LJ. The intersection of health and education to address school readiness of all children. Pediatrics 2018; 142: e20181126.
- 15. Hurley P, Noble K, Jackson J. Australian investment in education: early childhood education and care. Melbourne: Mitchell Institute, Victoria University; 2020. https://www.vu.edu.au/sites/default/files/australian‐investment‐in‐education‐ecec‐report‐mitchell‐institute.pdf (viewed Aug 2025).
- 16. Lycett K, Cleary J, Calder R, et al. A framework for the Future Healthy Countdown 2030: tracking the health and wellbeing of children and young people to hold Australia to account. Med J Aust 2023; 219 (Suppl): S3‐S10. https://www.mja.com.au/journal/2023/219/10/framework‐future‐healthy‐countdown‐2030‐tracking‐health‐and‐wellbeing‐children
- 17. Center on the Developing Child (2007). InBrief: The science of early childhood development. Cambridge (MA): Center on the Developing Child, Harvard University; 2007. https://developingchild.harvard.edu/resources/inbriefs/inbrief‐science‐of‐ecd/ (viewed Aug 2025).
- 18. Caspi A, Houts RM, Belsky DW, et al. Childhood forecasting of a small segment of the population with large economic burden. Nat Hum Behav 2016; 1: 0005.
- 19. Heckman JJ, Masterov DV. The productivity argument for investing in young children. Rev Agric Econ 2007; 29: 446‐493.
- 20. Australian Government Department of Education. Previous funding arrangements [website]. Canberra: Commonwealth of Australia, 2025. https://www.education.gov.au/early‐childhood/about/preschool/previous‐funding‐arrangements#toc‐what‐is‐the‐universal‐access‐national‐partnership (viewed Sept 2025).
- 21. Australian Government Department of Education. Budget 2024–25: Next steps to building universal early childhood education and care [website]. Canberra: Commonwealth of Australia, 2024. https://www.education.gov.au/early‐childhood/announcements/budget‐202425‐next‐steps‐building‐universal‐early‐childhood‐education‐and‐care (viewed Sept 2025).
- 22. Australian Government Department of Education. Fact Sheet ‐ Building Early Education Fund [website]. Canberra: Commonwealth of Australia, 2024. https://www.education.gov.au/about‐department/resources/building‐early‐education‐fund (viewed Sept 2025).
- 23. Australian Government Department of Education. Early Childhood Care and Development Policy Partnership [website]. Canberra: Commonwealth of Australia, 2025. https://www.education.gov.au/closing‐the‐gap/closing‐gap‐early‐childhood/early‐childhood‐care‐and‐development‐policy‐partnership (viewed Sept 2025).
- 24. Australian Government Department of the Prime Minister and Cabinet. New laws expand Paid Parental Leave — more support for working families with biggest expansion since 2011 [website]. Canberra: Commonwealth of Australia, 2024. https://www.pm.gov.au/media/new‐laws‐expand‐paid‐parental‐leave‐more‐support‐working‐families‐biggest‐expansion‐2011 (viewed Sept 2025).
- 25. Victorian Government. The Best Start, Best Life reforms [website]. Melbourne: State Government of Victoria, 2024. https://www.vic.gov.au/best‐start‐best‐life‐reforms (viewed Sept 2025).
- 26. Victorian Government. School Readiness Funding [website]. Melbourne: State Government of Victoria, 2025. https://www.vic.gov.au/school‐readiness‐funding (viewed Sept 2025).
- 27. Government of Western Australia. Funding for Early Childhood Education and Care in regional WA [website]. Perth: Government of Western Australia, 2024. https://www.wa.gov.au/government/media‐statements/Cook‐Labor‐Government/Funding‐for‐Early‐Childhood‐Education‐and‐Care‐in‐regional‐WA‐20240527 (viewed Sept 2025).
- 28. McArthur G, Sheehan Y, Badcock NA, et al. Phonics training for English‐speaking poor readers. Cochrane Database Syst Rev 2018; (11): CD009115.
- 29. Suggate SP. A meta‐analysis of the long‐term effects of phonemic awareness, phonics, fluency, and reading comprehension interventions. J Learn Disabil 2016; 49: 77‐96.
- 30. Torgeson CJ, Brooks G, Hall J. A systematic review of the research literature on the use of phonics in the teaching of reading and spelling. University of Sheffield, 2006.
- 31. Organisation for Economic Co‐operation and Development. PISA 2022 Results (Volume I): The State of Learning and Equity in Education. Paris: OECD Publishing, 2023. https://www.oecd.org/en/publications/pisa‐2022‐results‐volume‐i_53f23881‐en.html (viewed Sept 2025).
- 32. McCartan CJ, Roberts J, Jordan JA. Centre‐based early education interventions for improving school readiness: a systematic review. Campbell Syst Rev 2023; 19: e1363.
- 33. Australian Research Council. Medical Research Policy 2020.1. Canberra: Commonwealth of Australia, 2020. https://www.arc.gov.au/sites/default/files/2022‐09/ARC%20Medical%20Research%20Policy%20version%202020.1.pdf (viewed Sept 2025).
- 34. Health Data Research UK. Population Research UK prospectus. London: HDR UK, 2021. https://www.hdruk.ac.uk/wp‐content/uploads/2021/12/PRUK‐prospectus‐final.pdf (viewed Sept 2025).
- 35. European Commission. Horizon Europe. Brussels: European Commission, 2025. https://research‐and‐innovation.ec.europa.eu/funding/funding‐opportunities/funding‐programmes‐and‐open‐calls/horizon‐europe_en (viewed Sept 2025).
- 36. Klassen TP, Hartling L, Craig JC, Offringa M. Children are not just small adults: the urgent need for high‐quality trial evidence in children. PLoS Med 2008; 5: e172.
- 37. Gale C, Hyde MJ, Modi N, WHEAT Trial Development Group. Research ethics committee decision‐making in relation to an efficient neonatal trial. Arch Dis Child Fetal Neonatal Ed 2017; 102: F291‐F298.
- 38. Rose G. Sick individuals and sick populations. Int J Epidemiol 2001; 30: 427‐432; discussion 433‐434.
- 39. Cho SM, Serghiou S, Ioannidis JP, et al. Large pediatric randomized clinical trials in ClinicalTrials.gov. Pediatrics 2021; 148: e2020049771.
- 40. Zimmerman FJ. Population health science: fulfilling the mission of public health. Milbank Q 2021; 99: 9‐23.
- 41. Sanson A, Johnstone R; LSAC Research Consortium and FaCS LSAC Project Team. Growing Up in Australia takes its first steps. Family Matters 2004; 67: 46‐53.
- 42. Tayler C, Cloney D, Adams R, et al. Assessing the effectiveness of Australian early childhood education and care experiences: study protocol. BMC Public Health 2016; 16: 352.
- 43. Christian H, Nathan A, Trost SG, et al. Profile of the PLAY spaces and environments for children’s physical activity, sedentary behaviour and sleep (PLAYCE) cohort study, Western Australia. J Act Sedentary Sleep Behav 2025; 4: 7.
- 44. Telford RM, Olive LS, Telford RD. A peer coach intervention in childcare centres enhances early childhood physical activity: The Active Early Learning (AEL) cluster randomised controlled trial. Int J Behav Nutr Phys Act 2021; 18: 37.
- 45. Howard SJ, Vasseleu E, Neilsen‐Hewett C, Cliff K. Evaluation of the Preschool Situational Self‐Regulation Toolkit (PRSIST) program for supporting children’s early self‐regulation development: study protocol for a cluster randomized controlled trial. Trials 2018; 19: 64.
- 46. Hughes EK, Siero W, Gülenç A, et al. Generation Victoria (GenV): protocol for a longitudinal birth cohort of Victorian children and their parents. BMC Public Health 2025; 25: 20.
- 47. Silva DT, Hagemann E, Davis JA, et al. Introducing the ORIGINS project: a community‐based interventional birth cohort. Rev Environ Health 2020; 35: 281‐293.
- 48. Australian Government Department of Education. The Better and Fairer Schools Agreement (2025–2034). Canberra: Commonwealth of Australia, 2025. https://www.education.gov.au/recurrent‐funding‐schools/national‐school‐reform‐agreement/better‐and‐fairer‐schools‐agreement‐20252034 (viewed Sept 2025).
- 49. Wake M, Goldfeld S, Davidson A. Embedding life course interventions in longitudinal cohort studies: Australia’s GenV opportunity. Pediatrics 2022; 149 (Suppl): e2021053509R.
This article is included in a supplement which was funded by the Victorian Health Promotion Foundation (VicHealth). VicHealth is a pioneer in health promotion. It was established by the Victorian Parliament as part of the Tobacco Act 1987 and has a primary focus on promoting good health for all and preventing chronic disease.
Research at the Murdoch Children’s Research Institute is supported by the Victorian Government’s Operational Infrastructure Support Program. The funding sources had no role in the planning, writing or publication of the work.
No relevant disclosures.
Author contributions:
Melissa Wake: Conceptualization, writing – original draft, writing – review and editing. Jon Quach: Conceptualization, writing – review and editing. Jacqueline Davis: Conceptualization, funding acquisition, writing – review and editing.