





Mining activities have long been linked to health loss among occupationally exposed populations, leading to significant strengthening of workplace health and safety regulations. However, non‐occupational research is revealing increasingly robust evidence of both direct and indirect health risks, which are consistent with known emissions of toxic chemicals into the air, water and land during extraction, transportation and processing of mined materials. Epidemiological studies have identified a higher risk of cancer, circulatory and respiratory diseases, congenital anomalies and perinatal disorders in mining regions, globally.1 Most research has been conducted in the United States, China and Europe, with studies emerging from Africa, South America, South‐East Asia and India. Although Australia is one of the most important exporters of mined minerals and precious metals, research has focused mostly on environmental contamination and human health risk assessment of heavy metal byproducts such as lead and mercury.2,3,4,5 Limited epidemiological research in communities in mining areas in Australia hinders a comprehensive understanding of the public health impacts of mining, especially because of the magnitude and extent of mining activities in almost every Australian state and territory.
There were about 719 mines extracting solid materials in Australia in 2023;6 the majority in Western Australia, New South Wales and Queensland (Box 1). Gold, coal and iron ore mines account for 57% of total mining operations (30%, 17.5% and 9.8% respectively) with the remaining 43% mines extracting other minerals, including copper, mineral sands, silver, zinc, nickel, lead, bauxite, lithium, cobalt, asbestos and uranium.7 Although oil extraction is limited and onshore conventional gas reserves are dwindling, Australia's gas production and coal seam (unconventional) gas extraction is rapidly growing, with substantial gas resources and reserves in other states and the Northern Territory.
Mining, often identified as the most important industry in economic terms, has an EBIDTA (“earnings before interest, taxes, depreciation, and amortisation”, which is a measure of profitability to net income) of $274 676 million (the next two sectors are rental and real estate and construction, with EBIDTAs of $69 508 million and $58 801 million, respectively).8 However, the environmental, climate and health costs of mining are substantial. Globally, it has been estimated that, if environmental costs are deducted from mining‐generated income, the net economic gain is reduced by about 70%,9 whereas the value of statistical life costs exceeds the benefits of mining in coal mining areas in the United States.10 The environmental disruption of mining activities is associated with impacts from soil, air and water contamination. Higher concentrations of metals such as aluminium, iron, manganese, nickel and zinc, which exceeded the limits of Australia standards, have been measured in water from coal mine and gas extraction activities within, or discharging into, high conservation environments in several states.11,12,13 Nevertheless, a complete cost–benefit assessment of mining must include both occupational and public health impacts.
Since most research in Australia has focused on the health impacts of mining on workers, in this review we assess the evidence on the health impacts of mining in the general population, which encompasses the broader community. We implemented a systematic search of studies on the health impacts of mining and coal seam gas production in Australia, using three databases: Scopus, EMBASE and PubMed. We used a combination of title and abstract searches, keywords and MeSH terms to identify 29 and four studies on mining and gas production, respectively (Box 2). We then reviewed the systematic search findings in context with the scientific literature globally using a narrative review approach (the search strategy and selection process are provided in the Supporting Information). In the following sections, we address the health impacts of mining identified in the selected studies, discuss their findings with studies in other mining regions, and comment on the limitations, challenges and future directions for this research field (Box 3).
Epidemiolocal research on the human impacts of mining
Globally, epidemiological studies have assessed the health impacts associated with mining waste and emissions. Tailings from gold and silver mining are associated with high levels of heavy metals in soil and water near the mining activities, which can have a carcinogenic effect if ingested or inhaled. Multiple studies have estimated increased carcinogenic and non‐carcinogenic risk in both children and adults40,41 and in women of reproductive age who live in communities in proximity to gold mining.42
Mining of base, heavy and precious metals
In Australia, several studies have identified high concentration levels of cadmium, copper, iron, manganese, zinc, arsenic and lead in risk assessment analyses that evaluated bioavailability and risk reference dose models, or comparisons with international guidelines to estimate health risks.22,24,43 Consistently, analyses of human samples have identified high toenail arsenic concentrations in children in gold mining areas in Victoria, correlated with soil arsenic levels,23,25 supporting research on the potential pathways for systemic absorption of arsenic.44 A higher risk of all cancers and higher risk for melanoma, leukemia and prostate cancer in males and melanoma and colon cancer in females was associated with higher arsenic concentration in populations in proximity to gold mining areas in Victoria.26
In contrast to gold, which is mined mostly in Western Australia (60%), silver is mined as a byproduct of copper, zinc and lead, with the majority of mining operations located in Queensland.45 There are multiple studies assessing the health impacts associated with zinc–lead–silver mining in Australia, although most relate to lead‐linked impacts and in a few locations where severe contamination has prompted a social and public health response. Broken Hill in New South Wales has the world's largest zinc–lead–silver ore deposit, with subsequent lead contamination affecting local communities.15 Research has identified high lead concentrations in children's teeth and serum,17,18 supporting previous analyses that estimated an increased risk posed by the high concentration of lead and other metals including manganese, zinc, arsenic, lead2,16 and the implementation of a comprehensive plan for abatement of lead hazards in children's homes.
Although much debate on legacy sources (closed mines) being the dominant source of contamination hindered effective public health interventions in the early 1990s, recent research has found that contemporary mining activities are influencing the human exposure to lead within the Broken Hill general population.15 Studies of the human health impacts of lead in Australia are scarce. Nevertheless, epidemiological research has identified high concentration of lead in blood, urine and semen, which has been associated with impairment of semen quality and declining fertility in men,46 and intellectual disability (lower IQ scores) and impaired immune function of T lymphocytes and erythrocytes in children in lead mining areas.3,5 The studies in Broken Hill are consistent with research in other zinc–lead–silver mining regions in Australia, including the identification of high blood lead concentration in children in North Lake Macquarie in New South Wales and Mount Isa in Queensland.19,47
Coal mining
Despite Australia being the second largest coal exporter globally, with coal being mined for more than a century, the health impacts of coal mining on the general population have been barely investigated. Some studies have identified mental health and socially determined health conditions in communities in coal mining areas in Queensland, but these analyses did not use health data or bioindicators in a risk assessment context.48,49 Analyses in the Hunter Valley in New South Wales identified a higher rate of respiratory diseases compared with other non‐coal mining areas, but these differences were not statistically significant.34
More recent research has estimated an increased risk of hospitalisation due to circulatory and respiratory diseases in the Queensland general population using a Bayesian spatial and spatiotemporal framework to account for spatial dependency after adjusting for sociodemographic and environmental factors.32,33 These findings support previous studies that suggested that higher particulate matter concentrations in coal mining regions in Australia increase the risk of respiratory and circulatory diseases in communities in the vicinity of mining activities.50 This is consistent with the results from multiple studies in the United States and Europe which estimate a higher morbidity and mortality risk in communities in coal mining regions compared with non‐coal mining regions.1
Asbestos
A number of epidemiological studies on the impacts of asbestos mining have identified increased morbidity and mortality in communities close to these activities; however, most of these studies were done in Wittenoom, Western Australia.37,38,39 The higher exposure of these populations is associated with a higher risk of multiple respiratory and non‐respiratory cancers, especially in women and children, with early asbestos exposure in childhood also being associated with subclinical restrictive lung function.35,36,39 Despite the above studies evidencing significant human health impacts, the health effects of exposures to other mining wastes and emissions have not been estimated using human or clinical data and need to be assessed indirectly, mostly from risk assessment analyses.
Evidence from non‐human exposed studies
The assessment of the environmental properties associated with mining byproducts within close proximity to population centres, crops and potable water sources is an alternative way to assess the human health risks of mining activities. Risk assessment analyses of gold–copper mine tailings in central‐western New South Wales have identified levels of aluminium, copper and iron above recommended agricultural guidelines that affected Trifolium subterraneum and Phalaris aquatica growth, suggesting a biotoxic effect.51 This is consistent with risk assessments of other abandoned gold mine sites in New South Wales, which measured high concentrations of fine arsenic particle size arsenic (< 53 μm fraction).14 These particles have a high bioaccessibility and can be transferred easily through water and wind erosion, with concerns for potential inhalation and dermal contact via contaminated soils.21 Gold mining in other states is also associated with heavy metals pollution, such as contaminated soils in legacy gold mines in Maldon, Victoria, where arsenic and mercury concentrations exceeding safety environmental thresholds are considered a risk to the health of both humans and aquatic ecosystems.12
Lead exposure is prevalent in areas adjacent to local mining operations, especially in Broken Hill and Mount Isa, where soils have been chronically contaminated. Although the levels of lead in the air in Broken Hill appear to be declining, mine‐related emissions remain a cause of concern, with air lead concentrations being about 200 times greater than in other lead mining areas in New South Wales.4,15,16 In Mount Isa, lead concentrations in soil, dust and aerosols from areas adjacent to the copper and lead mines and smelters are derived from the Mount Isa lead–zinc ore bodies — an accumulation of solid and continuous mass of ore adhered to rocks.20 Multiple analyses of the lead isotopic composition indicate that atmospheric deposition of mine and smelter‐derived dusts are determinants of environmental contamination and form a significant pathway for lead exposures to the Mount Isa population.20,52,53
Analyses of coal mining areas, coal deposits and coal‐fired power stations in New South Wales have identified significant metal deposition of multiple potentially toxic agents such as copper, cobalt, zinc, arsenic, selenium, lead and aluminium, along with spheroidal carbonaceous particles13 and air emissions including particulate matter, sulphur dioxide and nitrogen oxides.50 Other risk assessment studies in the state have assessed the contamination of water from coal mining discharging into conservation environments. A study in the outer region of Sydney found sediment of arsenic, nickel and zinc in downstream coal mining discharge locations that exceeded the national guidelines.31 These analyses highlight the need to assess the management of coalmine run‐off and to regularly monitor sensitive receptors, such as natural water bodies, in combination with stronger regulatory measures to ensure safe and sustainable environmental and public health outcomes.
Health impacts of unconventional gas extraction
Australia's unconventional gas industry is the newest and least mature mining sector, commencing with new technological developments, notably horizontal drilling and hydraulic fracturing in the 1990s. Gas production in Queensland has surged since exports commenced in 2015. Profitable application of these technologies requires a vast land and water footprint containing thousands of wells and ancillary infrastructure close to homes and schools in densely populated areas (Box 4).54
The presence of this infrastructure has substantially increased emissions of nitrogen oxides, carbon monoxide, particulate matter, volatile organic compounds and formaldehyde in populated, high agricultural value areas of Darling Downs, Queensland, with a coincident increase in hospital admissions for severe circulatory, respiratory and cardiopulmonary conditions.27 Air quality testing in surrounding residential areas reveals exposures to toxic chemicals, including known carcinogens such as lead and cadmium.55 A community survey revealed higher than expected frequencies of symptoms known to be associated with these exposures, with 58% of surveyed residents indicating that their health had been negatively affected.54 Frequently reported symptoms included paraesthesia, headache, severe nose bleeding along with fatigue, weakness, attention deficit, eye and skin irritation, cough, rashes, joint pains, muscle pains and spasms, nausea and vomiting across all cohorts of the community, including children.54 Further studies found a higher risk of respiratory diseases in areas with unconventional gas operations compared with other rural areas with agricultural activities or other forms of mining.29 Beyond this evidence of acute effects, there are concerns about the long term public health impacts of chronic exposures that are currently not monitored.27 This is particularly relevant considering these analyses found up to a 467% increase in blood and immune diseases in children living in unconventional gas areas compared with rural areas.29
Despite the undisclosed large volume of chemical mixtures deployed in hydraulic fracturing affecting water aquifers and the air pollution associated with these activities, very few epidemiological studies have investigated the health impacts in exposed Australian communities.56 In contrast, there is an extensive body of research mostly in the United States, that establishes that people living in proximity to unconventional gas operations are at higher risk of multiple health consequences, including respiratory and circulatory diseases, mental health conditions, negative birth outcomes and congenital anomalies.57 These include higher frequencies of asthma exacerbations and hospitalisations in children in unconventional gas production areas in Pennsylvania and Texas58,59,60 and increased deaths and reduced life expectancy from cardiovascular, respiratory diseases and some cancers in Oklahoma and other states.61,62 Other studies also found higher hospitalisation rates for heart disease, respiratory and neurological disorders, and childhood cancers and immune deficiency disorders.27,28,58,63 Some of the most significant health risks are associated with pre‐birth exposure, which have a transgenerational impact. These risks include low birth weight and small for gestational age;64,65,66,67,68,69 pre‐term delivery and spontaneous abortion;65,70,71,72,73,74,75 birth defects, such as congenital heart valve defects, anencephaly, spina bifida and gastroschisis;64,76,77,78,79,80 and blood cancers, especially acute lymphoblastic leukaemia.81,82 This evidence provides a strong ground to consider that similar trends may be emerging in Australia, as populations increase their exposure to chemicals linked to oil and gas operations.
The list of impacts includes other health issues with profound effects and high public health costs, especially mental health conditions, more frequent traffic and pedestrian injuries and fatalities in unconventional gas production regions, increased incidence of sexually transmitted infections, and elevated risk of domestic and sexual violence associated with an influx of mobile workers into socially vulnerable areas.57 It is concerning that there are no peer‐reviewed human health impact assessments, accessible environmental baseline assessments or real‐time monitoring of environmental exposures, with no requirements for the industry to rectify these data gaps.83,84 As data for further analysis are inaccessible and the risks and severity of impacts remain incompletely defined, a comprehensive and effective application of the precautionary principle should be put in place until there is knowledge that these operations can be safely implemented in areas with potentially exposed populations.85
Future directions and conclusions
The findings of epidemiological and risk assessment studies in Australia coincide with global research in that mining is associated with a higher risk of morbidity and mortality in the general population in the vicinity of these industrial activities. The analyses of human tissues and samples indicate that neoplastic and non‐neoplastic diseases in exposed populations are mediated by a higher concentration of toxic mining byproducts such as cadmium, arsenic, mercury, lead and particulate matter among others.
We have highlighted some specific health conditions, but mining is also a determinant of social and economic issues that can have complex and deeper links with health impacts in communities in proximity to mining activities. Analyses of social and economic stress in mining communities have identified demographic imbalances, reflected in increasing antisocial behaviour, erosion of social capital, insecurity and crime, which are all associated with a higher risk of physical, mental and social health conditions.48,49 Aboriginal people are often at high risk of those conditions as well as deep cultural and spiritual losses from damage to their country land.57 The contrasting benefits derived from mining, mostly economic, versus its public health and other impacts support the concept of the so‐called “resource curse” (a paradox where a resource‐rich country underperforms economically), which should be extended to incorporate differences in health and social detrimental effects.86 This has been demonstrated in Australia, where long term analyses identify that resource booms tend to exacerbate inequality,87 and should be more relevant when considering the potential severe effects on vulnerable populations, especially children, and on reproductive health.88
A striking issue when assessing which health conditions are associated with mining in Australia is the scarcity of research studies, especially the analysis of human exposures using high quality health data. Although Australia is in a selected group of top research countries globally, the number and scope of studies in this area are limited to mostly non‐experimental associational analyses in a few mining regions, restricting timely and effective decision making to address these problems. This scarcity of research might relate to diverse factors, including deficiencies in public health and environmental legal frameworks, inefficient coordination between local and state government,47 outdated standards and exposure regulations,89 excess of political conflicting interest and incongruent environmental protection in the context of climate change,90 and the mining industry's role in pro‐industry lobbying.91 The academic sector, on the other hand, might tend to prioritise research in fields with higher returns in global rankings rather than environmental health problems.92 Another missing aspect is the association of mining with morbidity and/or mortality in Aboriginal and Torres Strait Islander people, which have not been investigated in epidemiological research except for social impact assessment analyses and government and academic reports. All mining in Australia is carried out on the Traditional Lands and Seas of Aboriginal peoples; often without their free, prior and informed consent. There is a small but growing grey literature that describes the severe social, emotional and spiritual impacts of mining on the Traditional Custodians of the impacted lands, who are often also the most affected by physical harms due to proximity and underlying conditions.57 Traditional Custodians feel a profound depth of social, emotional, cultural and spiritual loss as they witness the integrity of their Lands and Sea country broken and lose access and ability to fulfill their custodial responsibility to care for important sacred sites. They also suffer greatly when they lose their right to hand down the knowledge and stories about their Lands to their children, which threatens the survival of their cultural ways; however, these issues are rarely incorporated in epidemiological analyses of the health impacts of mining.33,48 All these factors severely affect the capacity of Australia to address the detrimental effects of mining in fair alignment with its economic benefits.
To overcome the multidimensionality of these limitations, it is critical to involve the mining industry, the community, the academic sector and the different levels of government. Analyses of the legal and economic challenges of fossil‐fuel resource developments in Australia have identified the need for an interdisciplinary approach, combining foreign investment, human rights, environmental law and land access regimes to balance the direct economic benefits with environmental and public health concerns.93,94 The coordinated participation of local and state governments is identified as a key factor to set governance arrangements to ensure the commitment of mining companies and other stakeholders to address mining‐specific impacts.95 These initiatives should be supported by strengthening current regulations, such as adherence to the health impacts assessment in all policies approach,96 and incorporation of epidemiological studies in well regulated processes, including environmental impact assessment.97
The academic and health sectors need to fill the knowledge gap of the health consequences of mining operations in the population in mining communities across the country. Although epidemiological research of diseases associated with environmentally widespread exposures such as soil and water contamination and air emissions are challenging, recent methodological approaches have been used to address research limitations and identify specific conditions associated with mining, such as cardiovascular and respiratory diseases in coal and unconventional gas mining areas in Queensland.29,30,32,33 Robust methodologies such as these spatial epidemiological analyses, Bayesian modelling to assess human health risks from multiple exposure pathways98 and target trial emulation99 can be used to develop a progressive understanding of the causal links between mining and morbidity and mortality in exposed populations. Further, both the public health and university sectors need to take responsibility for exercising and reinforcing the critical relevance of the precautionary principle and its use, given the high level of scientific uncertainty about the health risks of industrial activities such as mining and unconventional gas production.
Box 1 – Location of mine activities by type of mineral in Australia, 2023

Ag = silver; Al = aluminium; Au = gold; Cu = copper; K = potassium; Li = lithium; Mo = molybdenum; Ni = nickel; P = phosphorus; Pb = lead; REE = rare earth elements; Si = silicon; Ti = titanium; V = vanadium; Zn = zinc; Zr = zirconium. Source: Map designed with data from the Australian Operating mines 2023 dataset, Geoscience Australia.
Box 2 – Studies selected in the review by type of mining, health outcomes and methodological approach
|
Author (year) |
State (city/town) |
Type of mining |
Agent |
Health outcome or risk identified |
Analysis |
||||||||||
|
|
|||||||||||||||
|
Abraham et al (2018)12 |
Victoria |
Legacy mines |
Heavy metals |
Concentration exceeded safe standard |
Health risk assessment |
||||||||||
|
Fazle Bari et al (2021)14 |
NSW |
Legacy mines |
Arsenic |
Higer bioaccessibility in contaminated soil |
Health risk assessment |
||||||||||
|
Dong et al (2019)15 |
NSW (Broken Hill) |
Lead, silver, zinc |
Lead |
Concentration exceeded safe standard |
Health risk assessment |
||||||||||
|
Gillings et al (2022)16 |
NSW (Broken Hill) |
Lead, silver, zinc |
Lead |
Concentration exceeded safe standard |
Health risk assessment |
||||||||||
|
Gulson (1996)17 |
NSW (Broken Hill) |
Lead, silver, zinc |
Lead |
Higher concentrations in incisal and cervical sections of deciduous teeth (compared with controls) |
Health risk assessment |
||||||||||
|
Gulson et al (1994)18 |
NSW (Broken Hill) |
Lead, silver, zinc |
Lead |
Elevated blood lead levels |
Health risk assessment |
||||||||||
|
Gulson et al (2004)19 |
NSW (Broken Hill) |
Lead, silver, zinc |
Lead |
Elevated blood lead levels |
Health risk assessment |
||||||||||
|
Mackay et al (2013)20 |
Queensland (Mt Isa) |
Lead, silver, zinc |
Lead |
Concentration exceeded safe standard |
Health risk assessment |
||||||||||
|
Taylor et al (2014)2 |
NSW (Broken Hill) |
Lead, silver, zinc |
Arsenic, cadmium, lead |
Higher concentration in places accessible to children |
Health risk assessment |
||||||||||
|
Yang and Cattle (2015)4 |
NSW (Broken Hill) |
Lead, silver, zinc |
Lead |
Concentration exceeded safe standard |
Health risk assessment |
||||||||||
|
Hinwood et al (2004)21 |
Victoria |
Gold |
Arsenic |
Higher urinary inorganic concentrations |
Health risk assessment |
||||||||||
|
Martin et al (2018)22 |
Victoria |
Gold |
Arsenic |
Rapid lung bioaccessibility of arsenic in contaminated dust |
Health risk assessment |
||||||||||
|
Martin et al (2013)23 |
Victoria |
Gold |
|
Positive association of toenail Arsenic concentrations with concentration in soil |
Health risk assessment |
||||||||||
|
Noble et al (2010)24 |
Victoria (Stawell) |
Gold |
Arsenic |
Concentration exceeded safe standard |
Health risk assessment |
||||||||||
|
Pearce et al (2010)25 |
Victoria |
Gold |
Arsenic |
Concentration exceeded safe standard |
Health risk assessment |
||||||||||
|
Pearce et al (2012)26 |
Victoria |
Gold |
Arsenic |
Higher risk of all cancer and melanoma |
Epidemiological study |
||||||||||
|
McCarron (2018)27 |
Queensland (Darling Downs) |
Unconventional gas |
|
Increased acute circulatory admissions, compared with unconventional gas emissions in the same period |
Epidemiological study |
||||||||||
|
Werner et al (2017)28 |
Queensland |
Unconventional gas |
|
All‐cause hospital admissions |
Epidemiological study |
||||||||||
|
Werner et al (2018)29 |
Queensland |
Unconventional gas |
|
All‐cause and respiratory hospital admissions |
Epidemiological study |
||||||||||
|
Werner et al (2016)30 |
Queensland |
Unconventional gas |
|
Neoplasm and blood/immune diseases hospitalisations |
Epidemiological study |
||||||||||
|
Ali et al (2018)31 |
NSW |
Coal |
|
Concentration exceeded safe standard |
Health risk assessment |
||||||||||
|
Cortes‐Ramirez et al (2024)32 |
Queensland |
Coal |
|
Chronic circulatory and respiratory hospitalisations |
Epidemiological study |
||||||||||
|
Cortes‐Ramirez et al (2022)33 |
Queensland |
Coal |
|
Chronic circulatory and respiratory hospitalisations |
Epidemiological study |
||||||||||
|
Merritt et al (2013)34 |
NSW (Hunter Region) |
Coal |
|
General practice consultations and prescriptions (no significant differences with rural areas were found) |
Epidemiological study |
||||||||||
|
Franklin et al (2011)35 |
WA (Wittenoom) |
Asbestos |
|
Respiratory and non‐respiratory system cancers and reduced lung function |
Epidemiological study |
||||||||||
|
Reid et al (2007)36 |
WA (Wittenoom) |
Asbestos |
|
Higher rate of mesothelioma |
Epidemiological study |
||||||||||
|
Reid et al (2009)37 |
WA (Wittenoom) |
Asbestos |
|
Higher mortality rate due to mesothelioma |
Epidemiological study |
||||||||||
|
Reid et al (2013)38 |
WA (Wittenoom) |
Asbestos |
|
Increased “all cause” and “all cancer” mortality in females and males |
Epidemiological study |
||||||||||
|
Reid et al (2008)39 |
WA (Wittenoom) |
Asbestos |
|
Excess cancer mortality, including mesothelioma in females |
Epidemiological study |
||||||||||
|
|
|||||||||||||||
|
NSW = New South Wales; WA = Western Australia. |
|||||||||||||||
Box 3 – Key points on the health impacts of mining
- Mining byproducts are associated with health impacts in the general population in Australia and globally.
- Research in Australia consistently evidences multiple morbidity and mortality outcomes in the general population living in mining areas.
- Proximity to mining and exposure to toxic chemicals are associated with cancer and diseases of the respiratory, cardiovascular, immune and reproductive systems.
- Children and women in mining regions are especially vulnerable, with higher risk of perinatal conditions, and respiratory and blood and immune diseases.
- A multisectoral approach and stronger multilevel government coordination are required to address these public health impacts.
Box 4 – Distribution of coal seam gas wells (unconventional gas) in the Queensland Maranoa–Balonne–Condamine subregion, 2024*
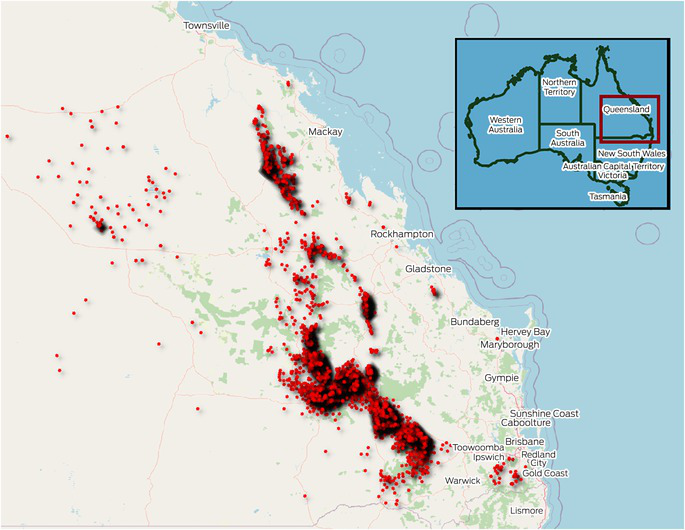
* Dark areas represent a high density of wells. Source: Map designed with data from the Queensland Spatial Catalogue — bore hole series, Department of Natural Resources and Mines, Manufacturing, and Regional and Rural Development (https://qldspatial.information.qld.gov.au/catalogue/custom/search.page?q=borehole).
Provenance: Commissioned; externally peer reviewed.
- Javier Cortes‐Ramirez1,2
- Ruby N Michael3
- Leisa‐Maree Toms1
- Melissa Haswell1
- 1 Queensland University of Technology, Brisbane, QLD
- 2 Centre for Data Science, Queensland University of Technology, Brisbane, QLD
- 3 Griffith University, Brisbane, QLD
Open access:
Open access publishing facilitated by Queensland University of Technology, as part of the Wiley – Queensland University of Technology agreement via the Council of Australian University Librarians.
No relevant disclosures.
Author contributions:
Cortes‐Ramirez J: Conceptualization, formal analysis, methodology, visualisations, writing original draft. Michael RN: Formal analysis, validation, writing review and editing. Toms LM: Formal analysis, validation, writing review and editing. Haswell M: Formal analysis, validation, writing review and editing.
- 1. Cortes‐Ramirez J, Naish S, Sly PD, Jagals P. Mortality and morbidity in populations in the vicinity of coal mining: a systematic review. BMC Public Health 2018; 18: 721.
- 2. Taylor MP, Mould SA, Kristensen LJ, Rouillon M. Environmental arsenic, cadmium and lead dust emissions from metal mine operations: implications for environmental management, monitoring and human health. Environ Res 2014; 135: 296‐303.
- 3. Wan C, Ma H, Liu J, et al. Quantitative relationships of FAM50B and PTCHD3 methylation with reduced intelligence quotients in school aged children exposed to lead: evidence from epidemiological and in vitro studies. Sci Total Environ 2024; 907: 167976.
- 4. Yang K, Cattle SR. Bioaccessibility of lead in urban soil of Broken Hill, Australia: a study based on in vitro digestion and the IEUBK model. Sci Total Environ 2015; 538: 922‐933.
- 5. Zhao ZY, Li R, Sun L, et al. Effect of lead exposure on the immune function of lymphocytes and erythrocytes in preschool children. J Zhejiang Univ Sci 2004; 5: 1001‐1004.
- 6. Australian Bureau of Statistics. Mineral and petroleum exploration, Australia. Canberra: ABS, 2024. https://www.abs.gov.au/statistics/industry/mining/mineral‐and‐petroleum‐exploration‐australia/jun‐2024 (viewed Oct 2024).
- 7. Hughes A, Britt A, Pheeney J, et al. Australia’s Identified Mineral Resources 2023. Canberra: Geoscience Australia, 2024. https://www.ga.gov.au/aimr2023 (viewed June 2025).
- 8. Australian Bureau of Statistics. Australian Industry, 2022–23. Canberra: ABS, 2024. https://www.abs.gov.au/statistics/industry/industry‐overview/australian‐industry/latest‐release#data‐downloads (viewed Sept 2024).
- 9. Cox B, Innis S, Kunz NC, Steen J. The mining industry as a net beneficiary of a global tax on carbon emissions. Commun Earth Environ 2022; 3: 17.
- 10. Hendryx M, Ahern MM. Mortality in Appalachian coal mining regions: the value of statistical life lost. Public Health Reports 2009; 124: 541‐550.
- 11. Ali A, Strezov V, Davies P, Wright I. Environmental impact of coal mining and coal seam gas production on surface water quality in the Sydney basin, Australia. Environ Monit Assess 2017; 189: 408.
- 12. Abraham J, Dowling K, Florentine S. Assessment of potentially toxic metal contamination in the soils of a legacy mine site in Central Victoria, Australia. Chemosphere 2018; 192: 122‐132.
- 13. Schneider L, Rose NL, Lintern A, et al. Assessing environmental contamination from metal emission and relevant regulations in major areas of coal mining and electricity generation in Australia. Sci Total Environ 2020; 728: 137398.
- 14. Fazle Bari ASM, Lamb D, Choppala G, et al. Arsenic bioaccessibility and fractionation in abandoned mine soils from selected sites in New South Wales, Australia and human health risk assessment. Ecotoxicol Environ Saf 2021; 223: 112611.
- 15. Dong C, Taylor MP, Zahran S. The effect of contemporary mine emissions on children’s blood lead levels. Environ Int 2019; 122: 91‐103.
- 16. Gillings MM, Fry KL, Morrison AL, Taylor MP. Spatial distribution and composition of mine dispersed trace metals in residential soil and house dust: Implications for exposure assessment and human health. Environ Pollut 2022; 293: 118462.
- 17. Gulson BL. Tooth analyses of sources and intensity of lead exposure in children. Environ Health Perspect 1996; 104: 306‐312.
- 18. Gulson BL, Davis JJ, Mizon KJ, et al. Lead bioavailability in the environment of children: blood lead levels in children can be elevated in a mining community. Arch Environ Health 1994; 49: 326‐331.
- 19. Gulson BL, Mizon KJ, Davis JD, et al. Identification of sources of lead in children in a primary zinc‐lead smelter environment. Environ Health Perspect 2004; 112: 52‐60.
- 20. Mackay AK, Taylor MP, Munksgaard NC, et al. Identification of environmental lead sources and pathways in a mining and smelting town: Mount Isa, Australia. Environ Pollut 2013; 180: 304‐311.
- 21. Hinwood AL, Sim MR, Jolley D, et al. Exposure to inorganic arsenic in soil increases urinary inorganic arsenic concentrations of residents living in old mining areas. Environ Geochem Health 2004; 26: 27‐36.
- 22. Martin R, Dowling K, Nankervis S, et al. In vitro assessment of arsenic mobility in historical mine waste dust using simulated lung fluid. Environ Geochem Health 2018; 40: 1037‐1049.
- 23. Martin R, Dowling K, Pearce D, et al. Ongoing soil arsenic exposure of children living in an historical gold mining area in regional Victoria, Australia: identifying risk factors associated with uptake. J Asian Earth Sci 2013; 77: 256‐261.
- 24. Noble RR, Hough RM, Watkins RT. Enrichment and exposure assessment of As, Cr and Pb of the soils in the vicinity of Stawell, Victoria, Australia. Environ Geochem Health 2010; 32: 193‐205.
- 25. Pearce DC, Dowling K, Gerson AR, et al. Arsenic microdistribution and speciation in toenail clippings of children living in a historic gold mining area. Sci Total Environ 2010; 408: 2590‐2599.
- 26. Pearce DC, Dowling K, Sim MR. Cancer incidence and soil arsenic exposure in a historical gold mining area in Victoria, Australia: a geospatial analysis. J Expo Sci Environ Epidemiol 2012; 22: 248‐257.
- 27. McCarron G. Air pollution and human health hazards: a compilation of air toxins acknowledged by the gas industry in Queensland’s Darling Downs. International Journal of Environmental Studies 2018; 75: 171‐185.
- 28. Werner AK, Cameron CM, Watt K, et al. Is increasing coal seam gas well development activity associated with increasing hospitalisation rates in Queensland, Australia? An exploratory analysis 1995–2011. Int J Environ Res Public Health 2017; 14: 540.
- 29. Werner AK, Watt K, Cameron C, et al. Examination of child and adolescent hospital admission rates in Queensland, Australia, 1995–2011: a comparison of coal seam gas, coal mining, and rural areas. Matern Child Health J 2018; 22: 1306‐1318.
- 30. Werner AK, Watt K, Cameron CM, et al. All‐age hospitalization rates in coal seam gas areas in Queensland, Australia, 1995‐2011. BMC Public Health 2016; 16: 125.
- 31. Ali AE, Strezov V, Davies PJ, Wright I. River sediment quality assessment using sediment quality indices for the Sydney basin, Australia affected by coal and coal seam gas mining. Sci Total Environ 2018; 616‐617: 695‐702.
- 32. Cortes‐Ramirez J, Mengersen K, Morawska L, et al. The hospitalisation risk of chronic circulatory and respiratory diseases associated with coal mining in the general population in Queensland, Australia. Sci Total Environ 2024; 949: 174989.
- 33. Cortes‐Ramirez J, Wraith D, Sly PD, Jagals P. Mapping the morbidity risk associated with coal mining in Queensland, Australia. Int J Environ Res Public Health 2022; 19: 1206.
- 34. Merritt TD, Cretikos MA, Smith W, Durrheim DN. The health of Hunter Valley communities in proximity to coal mining and power generation, general practice data, 1998‐2010. N S W Public Health Bull 2013; 24: 57‐64.
- 35. Franklin P, Reid A, Samuel L, et al. Respiratory morbidity of children exposed to crocidolite at Wittenoom, Western Australia. European Respiratory Journal 2014; 38(Suppl 55): 1055.
- 36. Reid A, Berry G, de Klerk N, et al. Age and sex differences in malignant mesothelioma after residential exposure to blue asbestos (crocidolite). Chest 2007; 131: 376‐382.
- 37. Reid A, Berry G, Heyworth J, et al. Predicted mortality from malignant mesothelioma among women exposed to blue asbestos at Wittenoom, Western Australia. Occup Environ Med 2009; 66: 169‐174.
- 38. Reid A, Franklin P, Olsen N, et al. All‐cause mortality and cancer incidence among adults exposed to blue asbestos during childhood. Am J Ind Med 2013; 56: 133‐145.
- 39. Reid A, Heyworth J, de Klerk N, Musk AW. The mortality of women exposed environmentally and domestically to blue asbestos at Wittenoom, Western Australia. Occup Environ Med 2008; 65: 743‐749.
- 40. Kamunda C, Mathuthu M, Madhuku M. Health risk assessment of heavy metals in soils from Witwatersrand gold mining basin, South Africa. Int J Environ Res Public Health 2016; 13: 663.
- 41. Ng JC, Ciminelli V, Gasparon M, Caldeira C. Health risk apportionment of arsenic from multiple exposure pathways in Paracatu, a gold mining town in Brazil. Sci Total Environ 2019; 673: 36‐43.
- 42. Marrugo‐Madrid S, Pinedo‐Hernández J, Paternina‐Uribe R, et al. Health risk assessment for human exposure to mercury species and arsenic via consumption of local food in a gold mining area in Colombia. Environ Res 2022; 215: 113950.
- 43. Vicente‐Beckett VA, McCauley GJ, Duivenvoorden LJ. Metals in agricultural produce associated with acid‐mine drainage in Mount Morgan (Queensland, Australia). J Environ Sci Health A Tox Hazard Subst Environ Eng 2016; 51: 561‐570.
- 44. Martin R, Dowling K, Pearce D, et al. Health effects associated with inhalation of airborne arsenic arising from mining operations. Geosciences 2014; 4: 128‐175; https://doi.org/10.3390/geosciences4030128.
- 45. Hughes A, Britt A, Pheeney J, et al. Australia’s Identified Mineral Resources 2022. Canberra: Geoscience Australia, 2023. https://www.ga.gov.au/digital‐publication/aimr2022 (viewed June 2025).
- 46. Tariba Lovaković B. Cadmium, arsenic, and lead: elements affecting male reproductive health. Curr Opin Toxicol 2020; 19: 7‐14.
- 47. Forbes M, Taylor MP. A review of environmental lead exposure and management in Mount Isa, Queensland. Rev Environ Health 2015; 30: 183‐189.
- 48. Petkova V, Lockie S, Rolfe J, Ivanova G. Mining developments and social impacts on communities: Bowen Basin case studies. Rural Society 2009; 19: 211‐228.
- 49. Lockie S, Franettovich M, Petkova‐Timmer V, et al. Coal mining and the resource community cycle: a longitudinal assessment of the social impacts of the Coppabella coal mine. Environ Impact Assess Rev 2009; 29: 330‐339.
- 50. Hendryx M, Higginbotham N, Ewald B, Connor LH. Air quality in association with rural coal mining and combustion in New South Wales Australia. J Rural Health 2019; 35: 518‐527.
- 51. Connick VJ, Raman A, Hodgkins DS, et al. Contents of Al, Cu, Fe, and Mo in Phalaris aquatica and Trifolium subterraneum grown on an unamended and amended gold‐mine tailings‐storage facility in central‐western New South Wales, Australia. Int J Min Reclam Environ 2010; 24: 195‐205.
- 52. Munksgaard NC, Taylor MP, Mackay A. Recognising and responding to the obvious: the source of lead pollution at Mount Isa and the likely health impacts. Med J Aust 2010; 193: 131‐132. https://www.mja.com.au/system/files/issues/193_03_020810/mun10320_fm.pdf
- 53. Sullivan M, Green D. Misled about lead: an assessment of online public health education material from Australia’s lead mining and smelting towns. Environ Health 2016; 15: 1.
- 54. McCarron GP, King D. Unconventional natural gas development: economic salvation or looming public health disaster? Aust N Z J Public Health 2014; 38: 108‐109.
- 55. Hook SE, Foster S, Althaus F, et al. The distribution of metal and petroleum‐derived contaminants within sediments around oil and gas infrastructure in the Gippsland Basin, Australia. Mar Pollut Bull 2023; 193: 115196.
- 56. Werner AK, Vink S, Watt K, Jagals P. Environmental health impacts of unconventional natural gas development: a review of the current strength of evidence. Sci Total Environ 2015; 505: 1127‐1141.
- 57. Haswell M, Hegedus J, Shearman D. The risks of oil and gas development for human health and wellbeing: a synthesis of evidence and implications for Australia. Sydney: University of Sydney, 2023. https://apo.org.au/node/324169 (viewed June 2025).
- 58. Buonocore JJ, Reka S, Yang D, et al. Air pollution and health impacts of oil and gas production in the United States. Environmental Research: Health 2023; 1: 021006.
- 59. Willis M, Hystad P, Denham A, Hill E. Natural gas development, flaring practices and paediatric asthma hospitalizations in Texas. Int J Epidemiol 2020; 49: 1883‐1896.
- 60. Bushong A, McKeon T, Regina Boland M, Field J. Publicly available data reveals association between asthma hospitalizations and unconventional natural gas development in Pennsylvania. PLoS One 2022; 17: e0265513.
- 61. Apergis N, Mustafa G, Dastidar SG. An analysis of the impact of unconventional oil and gas activities on public health: new evidence across Oklahoma counties. Energy Economics 2021; 97: 105223.
- 62. Li L, Dominici F, Blomberg AJ, et al. Exposure to unconventional oil and gas development and all‐cause mortality in Medicare beneficiaries. Nat Energy 2022; 7: 177‐185.
- 63. Blinn HN, Utz RM, Greiner LH, Brown DR. Exposure assessment of adults living near unconventional oil and natural gas development and reported health symptoms in southwest Pennsylvania, USA. PLoS One 2020; 15: e0237325.
- 64. Cairncross ZF, Couloigner I, Ryan MC, et al. Association between residential proximity to hydraulic fracturing sites and adverse birth outcomes. Jama Pediatr 2022; 176: 585‐592.
- 65. Caron‐Beaudoin E, Whitworth KW, Bosson‐Rieutort D, et al. Density and proximity to hydraulic fracturing wells and birth outcomes in Northeastern British Columbia, Canada. J Expo Sci Environ Epidemiol 2021; 31: 53‐61.
- 66. Tran KV, Casey JA, Cushing LJ, Morello‐Frosch R. Residential proximity to hydraulically fractured oil and gas wells and adverse birth outcomes in urban and rural communities in California (2006–2015). Environ Epidemiol 2021; 5: e172.
- 67. Hill EL. Shale gas development and infant health: evidence from Pennsylvania. J Health Econ 2018; 61: 134‐150.
- 68. Stacy SL, Brink LL, Larkin JC, et al. Perinatal outcomes and unconventional natural gas operations in Southwest Pennsylvania. PLoS One 2015; 10: e0126425.
- 69. Currie J, Greenstone M, Meckel K. Hydraulic fracturing and infant health: new evidence from Pennsylvania. Sci Adv 2017; 3: e1603021.
- 70. Casey JA, Savitz DA, Rasmussen SG, et al. Unconventional natural gas development and birth outcomes in Pennsylvania, USA. Epidemiology 2016; 27: 163‐172.
- 71. Hill EL, Ma L. Drinking water, fracking, and infant health. J Health Econ 2022; 82: 102595.
- 72. Whitworth KW, Marshall AK, Symanski E. Maternal residential proximity to unconventional gas development and perinatal outcomes among a diverse urban population in Texas. PLoS One 2017; 12: e0180966.
- 73. Cushing LJ, Vavra‐Musser K, Chau K, et al. Flaring from unconventional oil and gas development and birth outcomes in the Eagle Ford Shale in South Texas. Environ Health Perspect 2020; 128: 77003.
- 74. Deziel NC, Brokovich E, Grotto I, et al. Unconventional oil and gas development and health outcomes: A scoping review of the epidemiological research. Environ Res 2020; 182: 109124.
- 75. González DJX, Sherris AR, Yang W, et al. Oil and gas production and spontaneous preterm birth in the San Joaquin Valley, CA: a case–control study. Environ Epidemiol 2020; 4: e099.
- 76. McKenzie LM, Guo R, Witter RZ, et al. Birth outcomes and maternal residential proximity to natural gas development in rural Colorado. Environ Health Perspect 2014; 122: 412‐417.
- 77. Janitz AE, Dao HD, Campbell JE, et al. The association between natural gas well activity and specific congenital anomalies in Oklahoma, 1997–2009. Environ Int 2019; 122: 381‐388.
- 78. Tang IW, Langlois PH, Vieira VM. Birth defects and unconventional natural gas developments in Texas, 1999–2011. Environ Res 2021; 194: 110511.
- 79. Gaughan C, Sorrentino KM, Liew Z, et al. Residential proximity to unconventional oil and gas development and birth defects in Ohio. Environ Res 2023; 229: 115937.
- 80. Willis MD, Carozza SE, Hystad P. Congenital anomalies associated with oil and gas development and resource extraction: a population‐based retrospective cohort study in Texas. J Expo Sci Environ Epidemiol 2023; 33: 84‐93.
- 81. McKenzie LM, Allshouse WB, Byers TE, et al. Childhood hematologic cancer and residential proximity to oil and gas development. PLoS One 2017; 12: e0170423.
- 82. Clark CJ, Johnson NP, Soriano M, et al. Unconventional oil and gas development exposure and risk of childhood acute lymphoblastic leukemia: a case–control study in Pennsylvania, 2009–2017. Environ Health Perspect 2022; 130: 87001.
- 83. Dougall S. Host farmers: silence at the centre of the unconventional gas people‐place‐law nexus. Brisbane: Queensland University of Technology, 2024. https://eprints.qut.edu.au/249040/1/Shay%2BDougall%2BThesis%2B4.pdf (viewed June 2025).
- 84. Dougall S. Workplace health and safety (WHS) implications for farmers hosting unconventional gas (UG) exploration and production. Policy and Practice in Health and Safety 2019; 17: 156‐172.
- 85. Goldstein BD. The precautionary principle also applies to public health actions. Am J Public Health 2001; 91: 1358‐1361.
- 86. Savoia A, Sen K. The political economy of the resource curse: a development perspective. Annual Review of Resource Economics 2021; 13: 203‐223.
- 87. Bhattacharyya S, Williamson JG. Distributional consequences of commodity price shocks: Australia over a century. Review of Income and Wealth 2016; 62: 223‐244.
- 88. Wigley S. The resource curse and child mortality, 1961–2011. Soc Sci Med 2017; 176: 142‐148.
- 89. Taylor MP, Winder C, Lanphear BP. Australia’s leading public health body delays action on the revision of the public health goal for blood lead exposures. Environ Int 2014; 70: 113‐117.
- 90. Owens K. Breakthrough climate litigation positions courts to combat the health impacts of climate change. Med J Aust 2021; 215: 395‐397. https://www.mja.com.au/journal/2021/215/9/breakthrough‐climate‐litigation‐positions‐courts‐combat‐health‐impacts‐climate
- 91. Colagiuri R, Cochrane J, Girgis S. Health and social harms of coal mining in local communities. Beyond Zero Emissions, 2012.
- 92. Babones S. International student revenue and international rankings success: a case study of Australian university research strategies. Youth and Globalization 2022; 4: 56‐81.
- 93. Cassotta S, Cueva VP, Raftopoulos M. Australia: regulatory, human rights and economic challenges and opportunities of large‐scale mining projects: a case study of the Carmichael coal mine. Environmental Policy and Law 2021; 50: 357‐372.
- 94. Luke H, Emmanouil N. “All dressed up with nowhere to go”: navigating the coal seam gas boom in the Western Downs region of Queensland. The Extractive Industries and Society 2019; 6: 1350‐1361.
- 95. Everingham JA, Pattenden C, Klimenko V, Parmenter J. Regulation of resource‐based development: governance challenges and responses in mining regions of Australia. Environment and Planning C: Government and Policy 2013; 31: 585‐602.
- 96. Delany T, Harris P, Williams C, et al. Health impact assessment in New South Wales and health in all policies in South Australia: differences, similarities and connections. BMC Public Health 2014; 14: 699.
- 97. Cortes‐Ramirez J. Incorporating epidemiological studies into Integrated Environmental Health Impact Assessment of coal mining [PhD thesis]. Brisbane: University of Queensland, 2019; https://doi.org/10.14264/uql.2019.959.
- 98. Jiménez‐Oyola S, García‐Martínez MJ, Ortega MF, et al. Multi‐pathway human exposure risk assessment using Bayesian modeling at the historically largest mercury mining district. Ecotoxicol Environ Saf 2020; 201: 110833.
- 99. Hernán MA, Wang W, Leaf DE. Target trial emulation: a framework for causal inference from observational data. JAMA 2022; 328: 2446‐2447.
Summary